Thrombocytopenia is a symptom that manifests itself both in specific diseases of the blood system and in general somatic pathology, in some cases complicating drug therapy. Thrombocytopenia considered as a quantitative decrease in platelet count below 150 × 109/L [1–3]. For patients in critical condition, thrombocytopenia is a frequent symptom, its development is associated with many causes, it is an independent predictor of various complications and an unfavorable outcome [4–10]. Many authors describe a high prevalence of thrombocytopenia in intensive care units, Andreas Greinacher (2010) indicates 35–45 % of cases [4–8, 11]. The spread of the new coronavirus infection (NCI) COVID-19 has contributed to the aggravation of the course of a variety of diseases, especially in intensive care patients. Some authors point to thrombocytopenia as a characteristic sign of coronavirus infection [12–14]. The epidemiology of thrombocytopenia in patients in critical condition and in the conditions of a new coronavirus infection remains poorly understood and, therefore, the actual problem.
Objectives: To analyze the frequency of occurrence, severity, prognostic significance of thrombocytopenia in patients in critical condition without and with COVID-19 infection.
A retrospective cohort study was performed. Inclusion criteria: all patients of the Departments of Anesthesiology and Intensive Care of a multidisciplinary hospital: cardiological, neurological, general surgical, nephrological, obstetric, gynecological during normal operation (the period before the COVID-19 and during the period of care for patients with COVID-19). Patients of specialized onco-hematological resuscitation were not included, at the same time, patients of onco-hematological profile in general ICU were also included in the study. There were a total of 710 patients (314 in the period before the COVID-19 — group 1, 396 in the period during the COVID–19 — group 2). The groups did not differ in gender and age. The main characteristics of the patients are presented in Table 1.
Table 1. Characteristics of patients
| Indicator | Group 1 | Group 2 |
|---|---|---|
| Number of patients | 314 | 396 |
| Age, years | 59 (51.25–69.75) | 62 (52–72) |
| Distribution by gender, male/ female | 139/175 | 189/207 |
The platelet count was analyzed according to a Complete blood count (CBC) (ADVIA 2120i Hematology System, Siemens) performed in all patients from 7.00 to 8.00 on the day of the study. As part of a comprehensive assessment of hemostasis, coagulation assays (ACL TOP 500), viscoelastic hemostatic assays (TEG 5000) were performed; a clinical assessment including the identification of syndromes potentially leading to a decrease in the number of platelets, the presence and severity of hemorrhagic syndrome, as well as patient outcomes. The evaluation of these indicators was performed in the ICU at intervals of at least 2 weeks to prevent repeated inclusions of patients.
All patients from the non-infectious intensive care unit received therapy with low-molecular heparin in a preventive dose; in the infectious hospital — low-molecular heparin in a therapeutic dose. The exception was patients with severe hemorrhagic syndrome.
Thrombocytopenia was classified by severity into: mild — 100–150 × 109/L, moderate — 50–100 × 109/L, severe — < 50 × 109/L.
Accumulation, systematization of initial information and visualization of the results were carried out in Microsoft Office Excel 2016 spreadsheets. Statistical processing of the obtained data was carried out using the BioStat Pro 5.9.8 program. The variables were examined using visual (histograms) and analytical methods (Kolmogorov—Smirnov (KS) statistic) to determine the normality of the distribution. Quantitative data that did not obey the law of normal distribution were presented in the form of the median and the 25–75th percentile (Q1–Q3). Intergroup comparisons were carried out using the Mann—Whitney U-test. The calculation of the relative risk of death was carried out by constructing a four-field conjugacy table, based on the number of subjects with certain values of factorial and effective signs; the values of the boundaries of the 95 % confidence interval were estimated. Tests results were considered statistically significant when p ≤ 0.05.
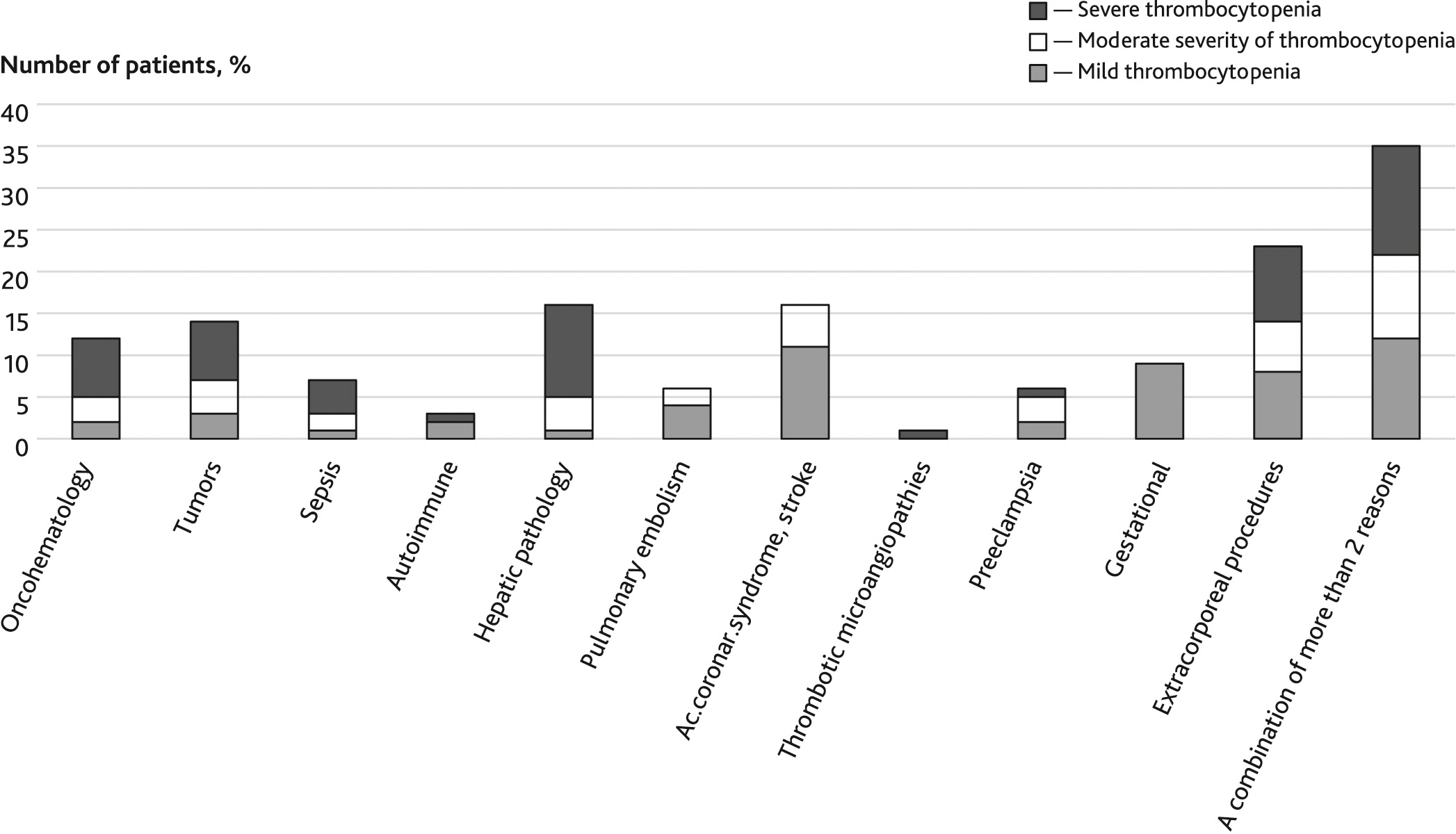
Period before COVID-19. Among 314 patients in group 1, 91 cases of thrombocytopenia were identified, which was 29 %. Severe thrombocytopenia among them was noted in 35 % (32 cases).
The most frequent thrombocytopenia occurred in patients receiving extracorporeal interventions. A mild form of thrombocytopenia was often observed in cardiology patients, neurological patients — 11 (12 %) and obstetric patients — 9 (9.8 %). Hepatic pathology, tumors, and sepsis were accompanied predominantly by profound thrombocytopenia. One patient (1.1 %) with thrombotic microangiopathy demonstrated severe thrombocytopenia. Autoimmune diseases (excluding immune thrombocytopenia, characterized overwhelmingly by profound thrombocytopenia; it did not occur in this sample) were less common. Pulmonary artery branch thromboembolism was detected in 6 (6.6 %) cases and was accompanied by mild to moderate thrombocytopenia. The causes and severity of thrombocytopenia are illustrated in Fig. 1.
Fig. 1. Causes and severity of thrombocytopenia before СOVID-19
Hemorrhagic syndrome minor in the form of hematomas in the vascular puncture area occurred in 12 (13.2 %) patients with tumors, sepsis, hepatic, cardiac pathology with mild and 10 (10.1 %) patients with moderate thrombocytopenia severity. Patients with cancer, sepsis (n = 12; 13.2 %) demonstrated severe thrombocytopenia accompanied by hemorrhagic diathesis, hematomas in the area of invasive interventions and spontaneous, but without severe hemorrhagic syndrome and did not require replacement therapy. In two patients (2.2 %) with gastrointestinal tumor process with diverticulitis, severe thrombocytopenia (below 20 × 109/L) was accompanied by massive gastrointestinal bleeding.
Period during COVID-19. Thrombocytopenia occurred more frequently than in patients outside COVID-19: in 209 of 396 Group 2 patients (52.8 %) and was more homogeneous in severity. Fig. 2 reflects the depth and causes of thrombocytopenia in this group. The most frequent cause of thrombocytopenia was a combination of sepsis, acute liver injury, performing extracorporeal procedures and specific drug therapy for COVID-19 infection.
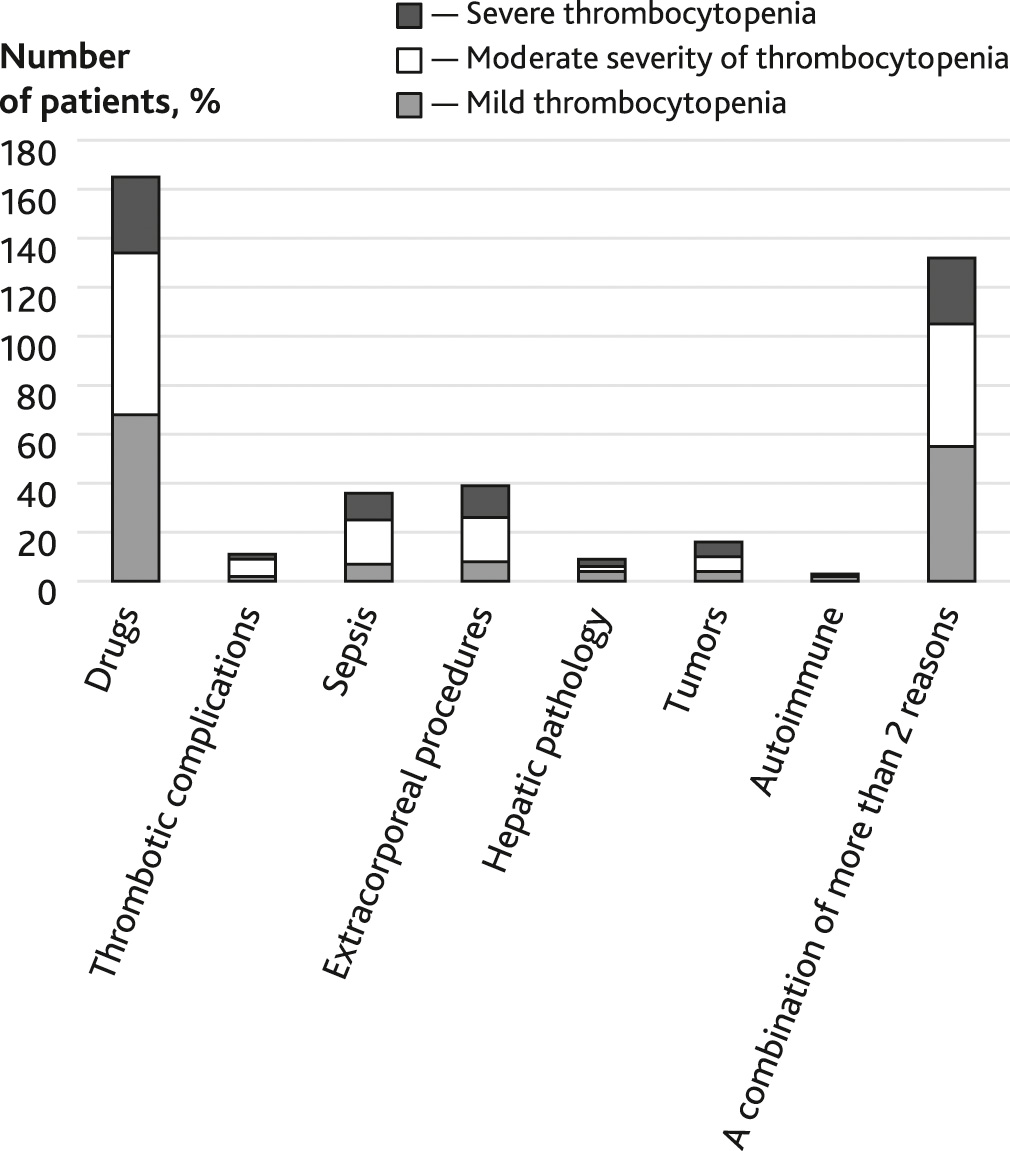
Fig. 2. Causes and severity of thrombocytopenia in an COVID-19 period
In this group of patients, according to our analysis, severe thrombocytopenia occurred less frequently: 20 % (42 cases) (Fig. 3). At the same time, significant hemorrhagic syndrome was detected in 13 (6.2 %) patients, which required erythrocyte replacement therapy: 5 (2.4 %) patients with a mild form, 2 (0.96 %) patients with a moderate form and 6 (2.9 %) patients with a severe form of thrombocytopenia.
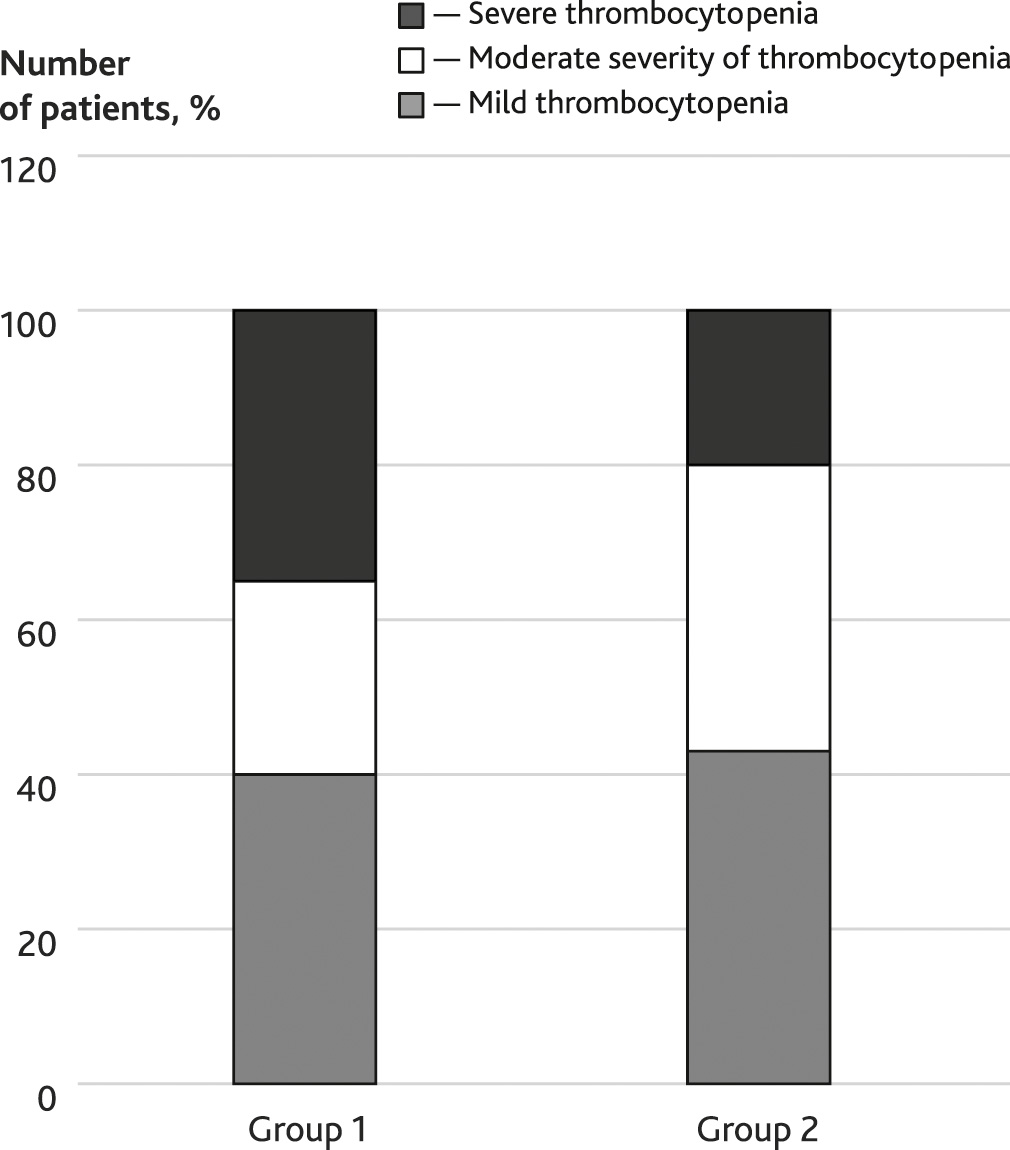
Fig. 3. Comparison of thrombocytopenia by severity before COVID-19 and during COVID-19 period
The distribution of the incidence of thrombocytopenia by severity is shown in Table 2.
Table 2. The frequency of occurrence of thrombocytopenia depending on the severity
| Severity of thrombocytopenia | The period before COVID-19 (group 1) | The period during COVID-19 (group 2) |
|---|---|---|
| Total cases of thrombocytopenia | 91* (29 %) | 209* (52.8 %) |
| Severe form | 32 (35 %) | 42 (20 %) |
| Moderate form | 23 (25 %) | 78 (37 %) |
| Mild form | 36 (40 %) | 89 (43 %) |
| * Absolute quantity. | ||
The calculated relative risk of death indicated a direct link between thrombocytopenia and an unfavorable outcome in critically ill patients. The presence of thrombocytopenia increased the risk of death 5.5-fold (95 % CI [2.979–10.031]) in group 1 and 1.54-fold (95 % CI [1.3–1.82]) in group 2.
There are several causes of thrombocytopenia. Traditionally, a pronounced decrease in the number of platelets is associated with a high risk of bleeding, both spontaneous and associated with performing invasive procedures. Platelets, as well as other blood cells and plasma proteins, "flow out" of the damaged vessel and are actively consumed to form a thrombus in the area of the damaged vessel. The risk of bleeding is always high in severe thrombocytopenia and increases in patients in the intensive care unit with mild or moderate COVID-19 in the presence of concomitant factors of hemostasis disorders: active fibrinolysis, platelet defect, performing invasive procedures, dilution against the background of massive infusion therapy, liver failure, etc. Timely monitoring of the effectiveness of anticoagulant therapy, if necessary, reducing the dose of drugs or a temporary break are necessary and sufficient in some cases preventive measures to prevent hemorrhagic complications.
The consumption and decrease in the number of platelets also occurs against the background of massive thrombosis [15]. In a number of patients, severe thrombocytopenia is a consequence of the development of various variants of vascular microthrombosis. A combination of thrombin depletion, deep thrombocytopenia and activation of fibrinolysis are observed in the development of disseminated intravascular coagulation syndrome (DIC) [16]. Severe infection with the outcome of sepsis, multiple organ failure and, against this background, pronounced consumption of blood cells, bone marrow dysfunction is a frequent companion of critical patients.
A slow and gradual decrease in the number of platelets may be caused by a deficiency of bone marrow, folate, vitamin B12. We observed patients with cardiological, neurological pathology with a mild form of thrombocytopenia and considered as its cause a decrease in bone marrow function, relative deficiency of vitamin B12 and folate, consumption against the background of the underlying disease: heart attack or ischemic stroke in patients predominantly elderly. A mild form of thrombocytopenia was present in the obstetric ICU in patients who were observed in the early postoperative period after cesarean section and anamnetically during the 3rd trimester of pregnancy. This variant of thrombocytopenia is classified as gestational. Many authors do not consider it a pathology, but a feature of the third trimester of pregnancy: it is not immune in nature, does not cause hemorrhagic complications, the number of platelets normalizes independently in the early postpartum period [17].
A sharp and rapid decrease in the number of platelets within 7–10 days indicates immune mechanisms, including those caused by heparin in the presence of indications for heparin therapy [10, 11, 18]. In our study, there were no laboratory-proven cases of immune thrombocytopenia, including heparin-induced (absence of antibodies to platelets and antibodies to heparin-platelet factor 4 complex).
The period during COVID-19 demonstrated a high incidence of thrombocytopenia: half of cases versus a third in non-infectious patients. The virus is an independent cause of a decrease in the number of platelets. This is due to several mechanisms [19–21]. The virus directly and through a cytokine storm affects the bone marrow, preventing the normal differentiation of hematopoietic cells, including megakaryocytes, triggers immune mechanisms of cell destruction and apoptosis [12, 15, 20]. Thrombopoietin production decreases, disrupting megakaryopoiesis [22]. Activated endothelium facilitates adhesion, promotes aggregation of platelets, neutrophils, monocytes. Local increased aggregation in the vessels of the lungs leads to micro-clots at the capillary level, stagnation of blood. Platelet adhesion with neutrophils facilitates platelet phagocytosis, improving platelet clearance in the spleen. The virus directly induces tissue factor expression by activating the coagulation cascade through increased thrombin generation; as well as activating monocytes and macrophages that express tissue factor [21]. As a result, microthrombosis increases with platelet consumption.
A great contribution to the development of thrombocytopenia was made by the effect of drugs. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), antibiotics, cytostatic drugs, heparins are a known cause of thrombocytopenia [3].
Severe infection with the outcome of sepsis, extracorporeal procedures and mechanical consumption of cells, acute liver damage, thrombosis, the above syndromes were detected in patients with varying degrees of thrombocytopenia.
At the beginning of the COVID-19 pandemic, many researchers pointed to the frequent occurrence of thrombotic complications in severe patients [13, 15, 23]. Further studies indicate that not only thrombosis, but hemorrhagic syndrome [14, 15], including spontaneous, is often present in these patients. This is confirmed by our current analysis. The concept of hemorrhagic complications in COVID-19 is also gaining importance and makes us reconsider the tactics of invasive interventions, anticoagulant therapy, substitution transfusion and laboratory evaluation. In the period during COVID-19, hemorrhagic syndrome was significantly more pronounced in patients with varying degrees of severity of thrombocytopenia. The appearance of bleeding, even with mild to moderate thrombocytopenia, was explained by a combined acute hepatic injury: in all patients with a pronounced violation of the regulation of fibrinogen synthesis, and in some cases with a decrease in the activity of prothrombin complex factors. Low fibrinogen concentration and thrombocytopenia lead to a significant violation of the formation of a physiological blood clot. These disorders have been repeatedly observed clinically and in the laboratory: a decrease in the activity of prothrombin complex factors according to coagulogram data, as well as an elongation of the start time of blood clotting (interval r) and a decrease in blood clot density (maximum amplitude) during thromboelastography.
Both in patients before COVID-19 and in patients during COVID-19, it was shown that a decrease in the number of platelets in critical patients is a risk factor for death. Confirmation of this was also found in the analysis of the literature [7, 9, 11]. But the relative risk of death in patients with COVID-19 turned out to be much lower than in patients of a multidisciplinary hospital, which speaks against including the number of platelets in a number of prognostic markers for a new coronavirus infection.
According to our data, thrombocytopenia in intensive care units of a multidisciplinary hospital (outside of work with COVID-19) occurred in 29 % of patients. The new coronavirus infection demonstrated an increase in the incidence of thrombocytopenia in critical patients, in the presented study to 52.8 %. Severe thrombocytopenia was more common in patients outside COVID-19 (35 % vs 20 %). In patients with coronavirus infection, thrombocytopenia was more often accompanied by a bleeding clinic (6.2 % vs 2.2 %), while it had less prognostic value as a criterion for an unfavorable outcome: the presence of thrombocytopenia increased the risk of death by 5.5 times (95 % CI [2.979–10.031]) in the period before COVID-19 and by 1.54 times (95 % CI [1.3–1.82]) during the period during COVID-19.
Disclosure. The authors declare that they have no competing interests.
Author contribution. All authors according to the ICMJE criteria participated in the development of the concept of the article, obtaining and analyzing factual data, writing and editing the text of the article, checking and approving the text of the article.
Ethics approval. Ethic approval by the local Ethical Committee is not required for current study design.